Bunionectomy
[masterslider id=”8″]
Bunions are progressive bone deformities of the foot that often cause recurring or chronic inflammation, irritation, and pain that require surgical correction. Surgical removal of a bunion is called a bunionectomy. However, there are multiple types of bunionectomies, each designed to resolve different structural changes caused by the deformity.
Bunion surgeries fall into two major categories:
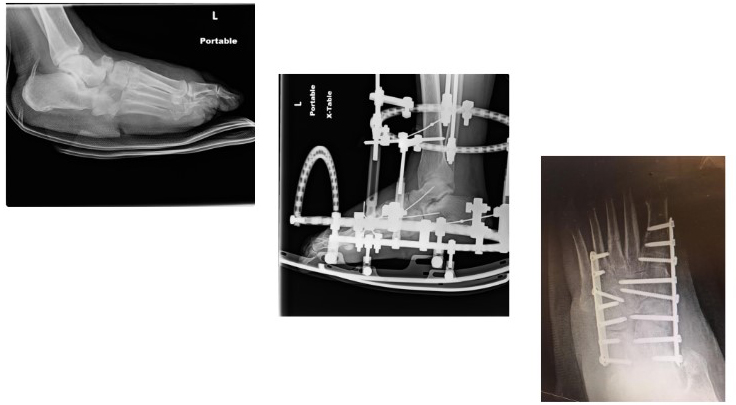
- Head procedures that treat the big toe joint. In a head procedure bunionectomy, the bone is cut just behind the joint, moved into its proper position, and fixed in place with a screw or pin. Head procedures are often used for patients who cannot be immobilized for long periods of time.
- Base procedures concentrate on the bone near or behind the big toe joint. Different types of base procedures are conducted depending on the nature of the deformity. These range from cutting a wedge out of the bone and splitting it so that it can be moved into its proper position; making a semi-circular cut and rotating the bone into its correct position; or fusing the joint. Ligaments inside and outside the toe may also be treated during a base procedure.
There are three important factors that impact the success of bunion surgery:
- Choose a surgeon with extensive experience with bunionectomies. Because a deep understanding of the biomechanics of each patient’s foot, as well as the intricacies of each surgical option, is needed, surgeons with more experience at doing bunionectomies are better able to help each patient achieve the best outcome.
- Be realistic in your expectation about what a bunionectomy can accomplish. No physician can guarantee that a bunion won’t recur or that a patient will be absolutely pain-free. Additionally, because of the complexity of the foot structures impacted by a bunion, patients may never be able to wear normal or slender shoes. Bunion surgery can reduce or eliminate the bone deformity, improve foot alignment and function, and prevent damage to other toes, but it does have its limitations. Be sure you understand all the possibilities before opting for this surgery.
- Bunion surgery is not a magic bullet. Surgery alone may not be all that is needed to achieve your best outcome. After surgery, many patients experience long healing and recovery times and often have to spend time in physical therapy. Additionally, you may need a corrective orthotic device on an ongoing basis.
What to Expect
Most bunions surgeries today are performed on an outpatient basis at a surgical center or hospital. Set aside the entire day for the surgery, although you may only be at the facility for a half day.
Prior to the surgery, patients will need to make some preparatory arrangements. These include:
- Seeing your Primary Care Physician (PCP) to make sure any other health conditions are stabilized prior to surgery and to document your complete medical history, which can then be given to the foot surgeon.
- Arranging your schedule to make sure you don’t need to take any long trips for at least two to three weeks following the surgery.
- Lining up another person to drive you home and stay with you for the first 24 hours after the surgery.
- Stopping the use of any anti-inflammatory medications, such as aspirin, ibuprofen, or acetaminophen, for five to seven days before the surgery.
The night before the surgery, you will not be able to eat or drink anything after midnight. You should also wash your foot the night before and morning of the procedure to help reduce surrounding bacteria and prevent infection.
Bunion surgery is usually performed with a local anesthetic and is administered by an anesthesiologist. This may be combined with sedation medication to put you into “twilight” so that you are fully relaxed. After the surgery, patients are often given a long-acting anesthetic and pain medication, which is why someone else must drive the patient home.
The type of procedure you have will determine the degree to which you can put weight on the foot immediately after the surgery. Some patients, particularly those having base procedures, may have to use crutches; others may be sent home wearing a surgical shoe. The foot will be covered in a dressing, which you will need to keep dry for up to two weeks or until the sutures are removed.
During the first week after surgery, you will need to keep the foot elevated as much as possible. Ice packs also should be applied for the first three to four days to reduce swelling. Limited ambulation or walking is required over the first two weeks to promote healing. Most patients also are instructed on some basic exercises that need to be performed daily.
Sutures are generally removed about two weeks after the surgery in the doctor’s office. Once the sutures are removed, you can bathe and shower normally, but will still need to wear a dressing over the wound to keep it clean and prevent infection.
By the third or fourth-week post surgery, swelling generally subsides enough for the patient to begin wearing a wide athletic shoe. It is important to continue daily exercises. If recommended, physical therapy may be initiated at this time. Once the wound has completely closed, you can use lotions to soften the skin in the surgical area.
By week five after the surgery, you will be able to walk short distances and do mild fitness activities. Continue following your surgeon’s instructions for increasing exercise and activities until you are back to normal.









 and impairment of the immune system is also likely to occur.
and impairment of the immune system is also likely to occur.